डाउनलोड प्रस्तुति
प्रस्तुति लोड हो रही है। कृपया प्रतीक्षा करें।

1
CPAP - INFLATION OF ATELECTATIC LUNG Dr. Rakesh kotha Associate professor of neonatology Niloufer hospital

2
VENTILATOR USUALLY DELIVERS INSPIRATION OR EXPIRATION PRINCIPLE NOSE =HUMIDIFIER LUNGS=VENTILATOR MORE INVASIVE TO MORE EFFECTIVE LESS INVASIVE

5
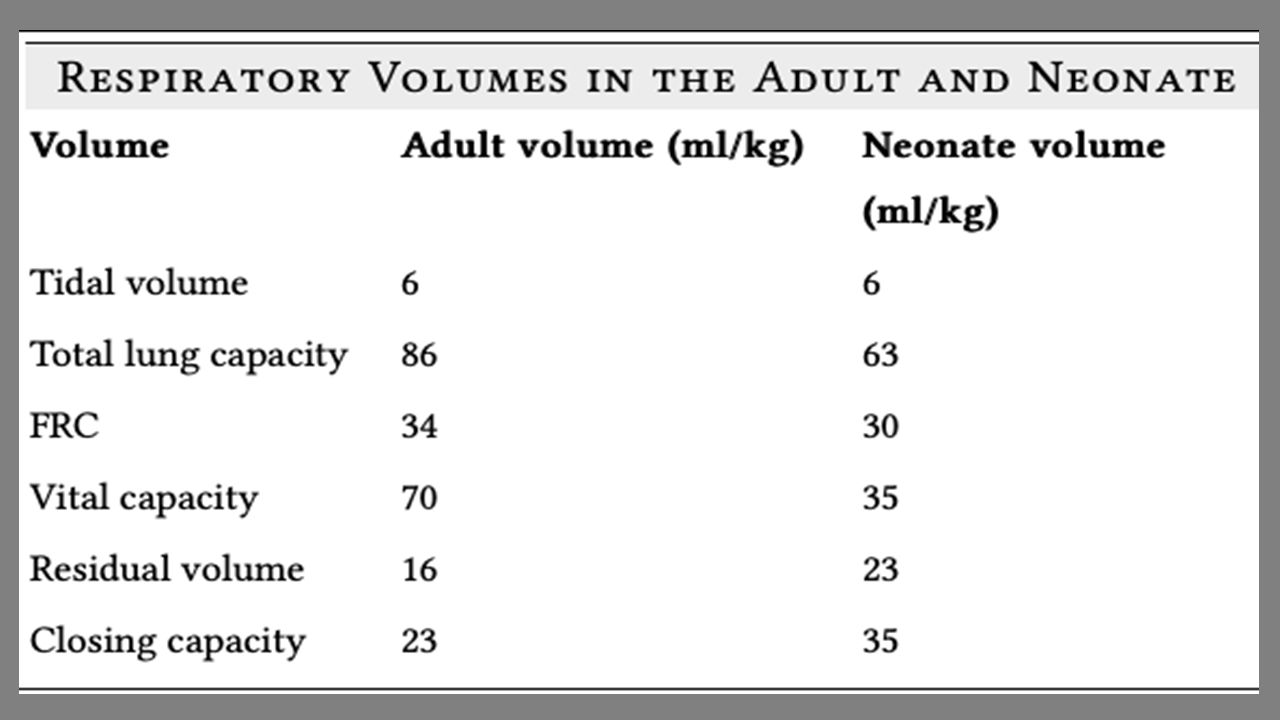
PEEP FRC < CV( neonates)
")
6
Where does CPAP stand? Ventilator NIPPV CPAP HHHFNC Low flow 02

7
does not require an ETT permits spontaneous breathing continuous pressure PEEP OBSERVE GRUNT FRC O2 ET

8
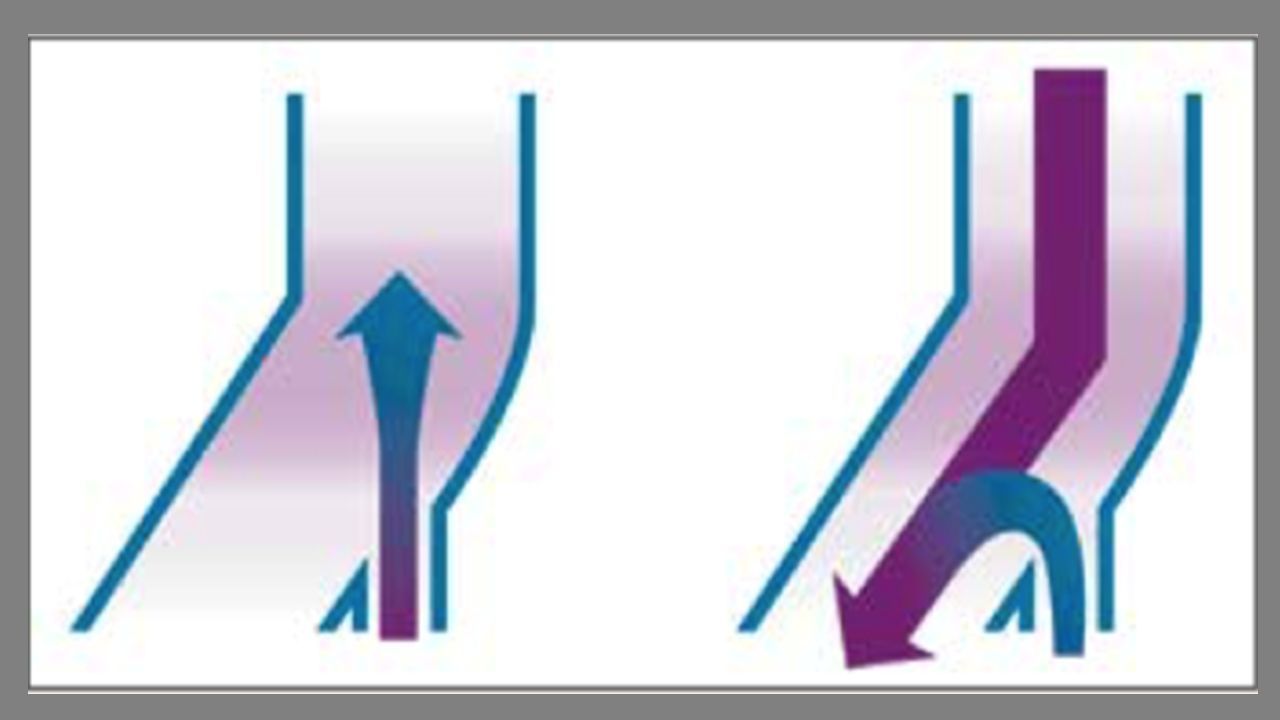
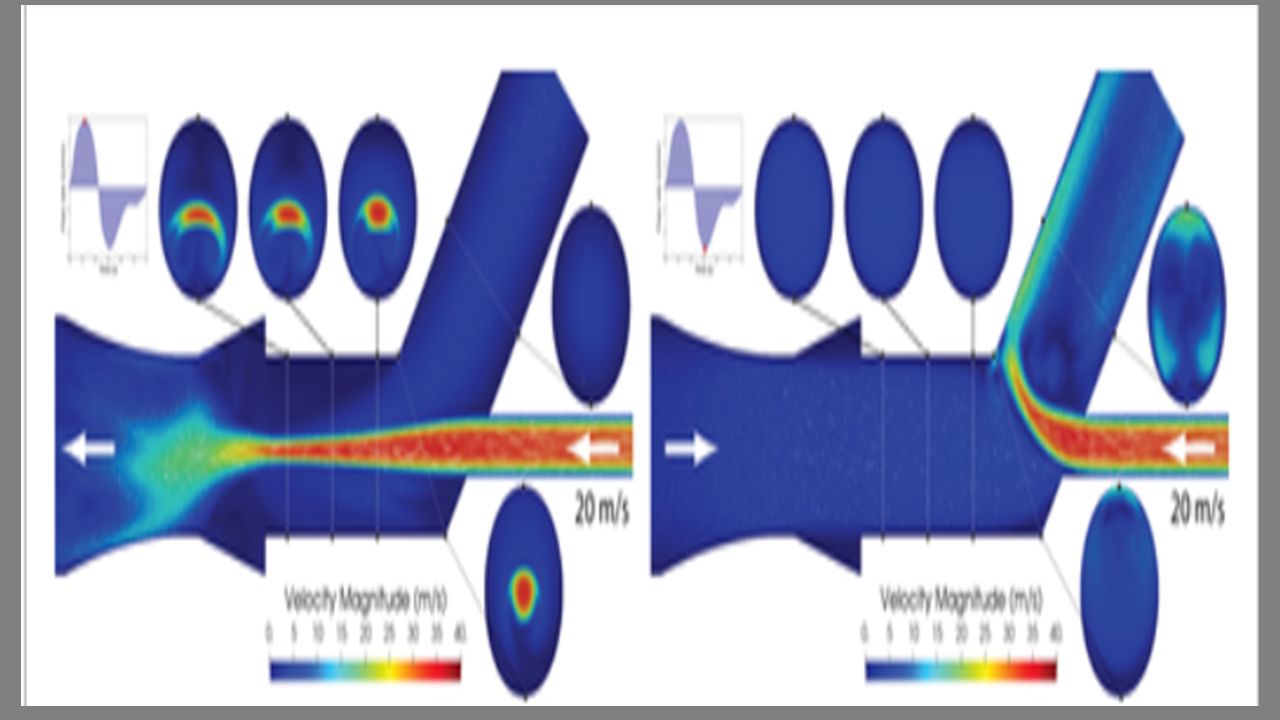
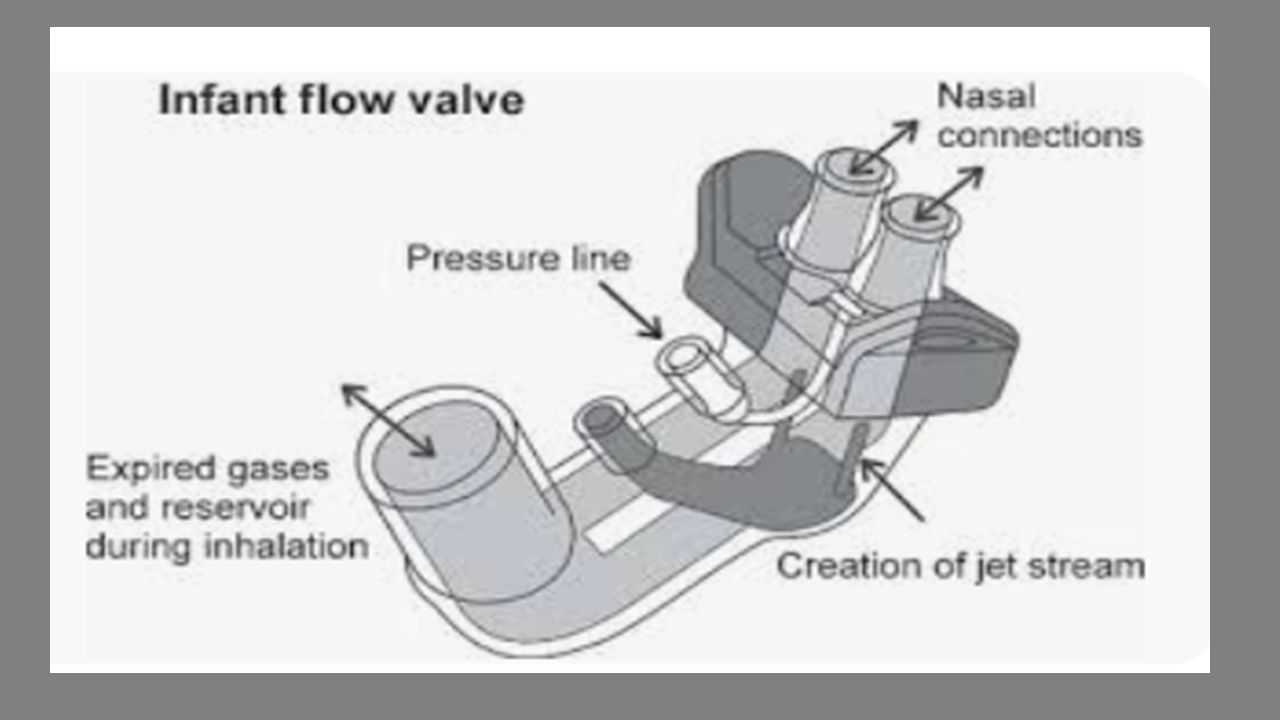
Types 1. Continuous flow CPAP – Bubble CPAP Ventilator CPAP 2. Variable flow CPAP Infant flow driver Pressure delivered at nose Expiration is passive

9
Any signs of significant respiratory distress Active <500gm Diseases with low functional residual capacity (FRC): SAS (APGAR) Indications
: SAS (APGAR) Indications")
10
Respiratory Distress Syndrome (RDS) Transient Tachypnoea of the newborn (TTN) Post extubation Tracheomalacia Apnoea of prematurity Pulmonary oedema
 Transient Tachypnoea of the newborn (TTN) Post extubation Tracheomalacia Apnoea of prematurity Pulmonary oedema")
11
PEEP= CDP facilitates gas exchange maintains functional residual capacity (gas for respiration) reduction of airway collapse by decreased airway resistance splinting of the pharyngeal airway to avoid obstruction HB reflex
 reduction of airway collapse by decreased airway resistance splinting of the pharyngeal airway to avoid obstruction HB reflex")
12
PEEP principles keeping surfactant on alveolar surface and reduction of alveolar oedema reduced work of breathing (Half dilated) improvement in ventilation-perfusion ratio and decreased intrapulmonary shunting OPEN LUNG CONCEPT(50%)
 improvement in ventilation-perfusion ratio and decreased intrapulmonary shunting OPEN LUNG CONCEPT(50%)")
13
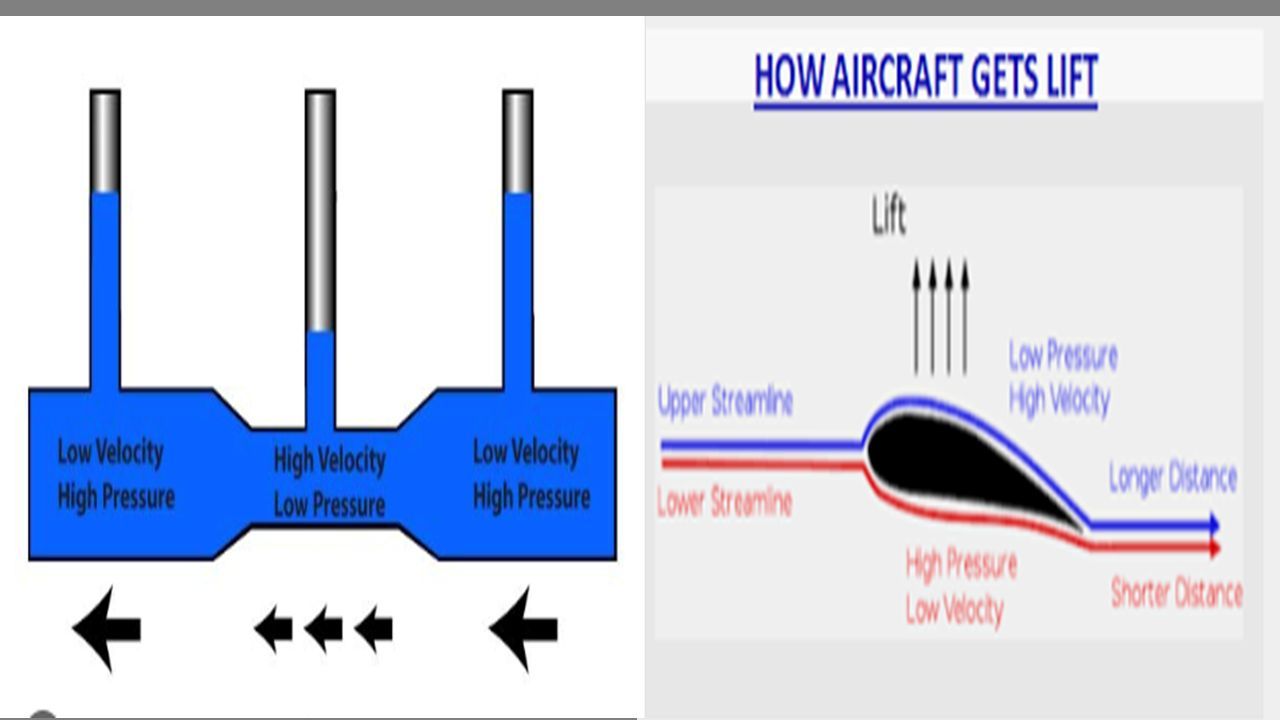
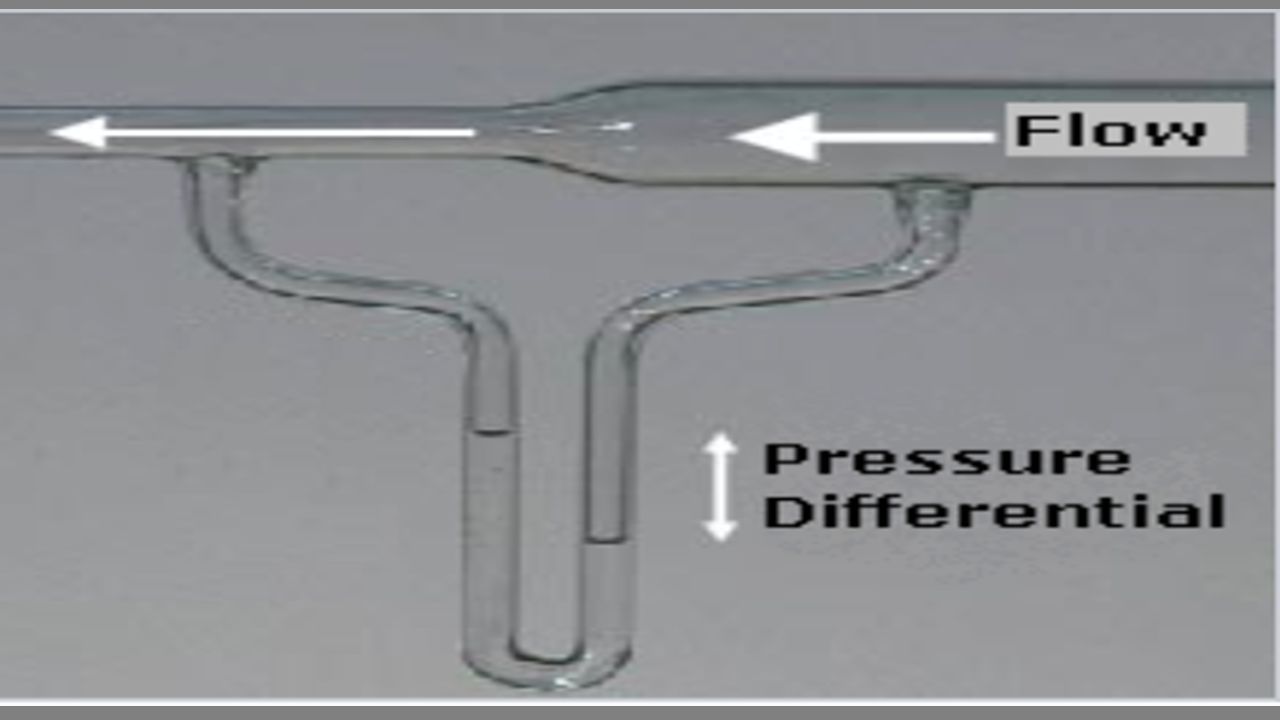
P=2T/r Recruitment

14
Contraindications: Upper airway abnormalities - choanal atresia, cleft palate, unrepaired trachea-oesophageal fistula,MAS Congenital Diaphragmatic hernia pre surgical repair

15
Attach only after optimum heating of humidifier NOSE

16
Circuit 37 C 100 % RH AA P? >8L

17
A34C 70 RH to 37 C 100 RH Adequate? AH RH

18
MORE BUBBLES ?(5 lit enough) CO 2 elimination &Surfactant secretion How to test CPAP delivering adequately ( ex:prongs will touch the nose) Humidification adequate ? (Water column will increase) Which type of water Open mouth
 Which type of water Open mouth.")
19
Ventilator CPAP Same circuit CPAP Hudson prongs/ mask (SIZE OF NARES AND DISTANCE) PIP? EXPIRATION =Passive?

27
Initiation CPAP 5cm Flow 5 L Fio2 50% (30%) spo2 92-95% Increase : 8cm H20 Cease : 4 cm h20 Fio2<30% Comfortable 5/5/5/5
 spo % Increase : 8cm H20 Cease : 4 cm h20 Fio2<30% Comfortable 5/5/5/5")
28
Escalation And Weaning And Titration Rule of Propotion PEEP 5 FiO2 50% Retractions=PEEP

29
Ten questions 1. What pressures to use ? 5 or 6 cm 2. Upto what Fio2 can I keep on CPAP ? 50 /60% 3. At what Flow ? 5-8 L/min 4. How much bubbling? Just enough(TURBULENT) 5. Should I worry about pneumothorax ? Yes
 5. Should I worry about pneumothorax . Yes.")
30
6. Should I do ABG daily ? No 7. What pco2 can I accept ? 50 mm Hg 8. When to wean ? Comfortable, Fio2<30%, PEEP 4/5, ABG normal 9. Can I feed, KMC ? Yes. Yes Yes 10. Is nursing care important ??

31
Interface Binasal prongs ETT ( Nasphra yngeal ) MaskChinstrap pacifier
 MaskChinstrap pacifier")
32
Nose Injury,Distance,should not dilate

33
Evidence CPAP with early rescue surfactant Less intubation Less surfactant Less mortality COIN/CURPAP/ SUPPORT /VON DRM

34
CPAP does not maintain oxygen saturation > 90% SAS score > 6 despite being on 50% oxygen and PEEP of 6 cm H2O if a neonate develops > 2 episodes of apnoea needing stimulation or positive pressure ventilation in 24 h Failure

35
Flow has to be altered to ensure proper bubbling It is difficult to detect high flow which can lead to over distension of the lungs Ossillations?

इसी तरह की प्रस्तुतियाँ



 हमारे चौथे इमाम>")


>")
![sf]if tyf n]vf lgoGqs sfof{no, nlntk'/](/88/15616961/big_thumb.jpg "sf]if tyf n]vf lgoGqs sfof{no, nlntk'/>")